
4.TIBC,TSAT
TIBC は,トランスフェリンに結合可能な鉄量を示し,血清トランスフェリン総量に相関する。
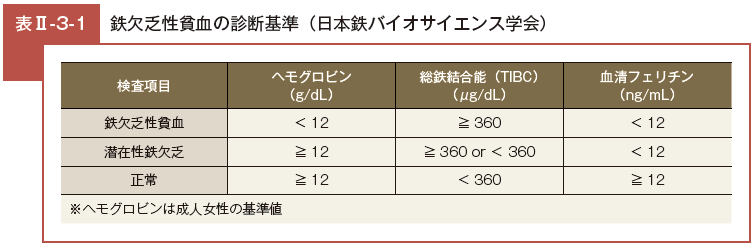
したがって,「TIBC = 不飽和鉄結合能(unsaturated iron binding capacity: UIBC)+ 血清鉄」となり, TIBC の正常値はおおよそ 240 〜 400μg/dL である。
TIBC は鉄欠乏において増加し,前述の血清フェリチンに次いで TIBC も特異性が高いが5),栄養状態・加齢・炎症により低下するため注意が必要である。
TIBC と血清鉄の比で示される TSAT は「血清鉄 /TIBC × 100%」で計算され,鉄欠乏の評価に用いられることがある。
正常値は 25 〜 30% であるが,鉄欠乏の進展に伴う血清鉄低下・TIBC 増加の結果,TSAT は低下する。これが 16% 以下となれば鉄欠乏が示唆される11)12)。
TSAT は,血清フェリチンと並び鉄欠乏の診断に有用であり,特に炎症状態などの存在により血清フェリチン値に信頼のおけない状況下で参考となる。
5.可溶性トランスフェリンレセプター
血清中の可溶性トランスフェリンレセプターの測定は鉄欠乏の診断にも有用であることが知られてきたが,保険診療上の制約があって,わが国では広く行われていない。
造血能のよい指標とされ,溶血性貧血のような赤芽球過形成を示す状態では高値を示す。
鉄欠乏でも初期から増加することが知られており13)14),可溶性トランスフェリンレセプターと血清フェリチンの対数値(log 血清フェリチン)の比が 1.5以上であれば鉄欠乏性貧血が疑われ,1.5 未満であれば慢性疾患に伴う貧血が考えられる11)。
6.その他
一般検査として確立されていないが,鉄欠乏の診断において注目されている検査として,網赤血球ヘモグロビン含量が挙げられる15)。
本項目は自動分析装置で簡便に測定することができ,鉄欠乏性貧血の診断だけでなく,血液透析患者へのエリスロポエチン投与による赤血球産生刺激に伴う鉄不足状態の把握に有用であるとして,英国のガイドラインでは推奨されている16)。
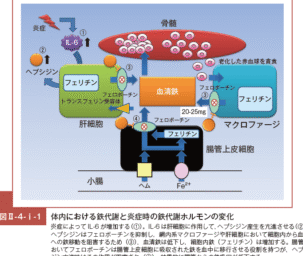
また,生体内の鉄制御に重要なヘプシジン(他項参照)も鉄欠乏性貧血では低下し,鉄の補充により回復しうる17)。ヘプシジンもよいマーカーとして期待されるものの,さらなる検討が必要である。
末梢血の血液像も診断上有用であり,鉄欠乏性貧血では一般に中心の色素を欠き(central pallor),リング上で厚みの足りない像を示す(leptocyte: 菲薄赤血球)。
また血球の大小不同(anisocytosis)や形の変形した赤血球(poikilocytes)を認めることもある。
網状赤血球は通常正常値〜やや増加する程度であるが,鉄剤治療時には急激に増加しうる。
骨髄検査は侵襲が高いため鉄欠乏性貧血が疑われる症例では通常施行しないが,鉄欠乏の診断における gold standard である。典型例では赤芽球系過形成で,健常者では 30 〜 50% みられる鉄可染性の赤芽球(sideroblast: 鉄芽球)が 10% 以下まで著減している12)。
鉄欠乏性貧血,慢性疾患に伴う貧血における各検査値の変動については「慢性疾患に伴う貧血」の項を参照。
文献
- Lewis Reference ranges and normal values. in Lewis SM, Bain BJ, Bates I (eds): “Dacie and Lewis Practical Hematology”, 9th ed, Churchill Livingstone, London, 2001, 9-18.
- 内田立身 . 鉄欠乏性貧血の治療指針 . 日本鉄バイオサイエンス学会治療指針作成委員会編 . 鉄剤の適正使用による貧血治療指針 . 改訂第 2版 . 札幌 , 響文社 , 2009. 10-17.
- Cook JD. Clinical evaluation of iron deficiency. Semin Hematol. 1982; 19: 6-18.
- Niitsu Y, Kohgo Y, Yokota M, et al. Radioimmunoassay of serum ferritin in patients with Ann N Y Acad Sci. 1975; 259: 450-452.
- Fielding Serum iron and iron binding capacity. Iron edited by Cook JD, Churchill Livingstone, New York; 1980, 15-43.
- Lipshitz DA, Cook JD, Finch CA. A clinical evaluation of serum ferritin as an index of iron stores. N Engl J 1974; 290: 1213-1216.
- WHO: WHO guideline on use of ferritin concentrations to assess iron status in individuals and populations. 2020 April.
- Mast AE, Blinder MA, Gronowski AM, et al. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin Chem. 1998; 44: 45-51.
- Camaschella Iron deficiency. Blood. 2019; 133: 30-39.
- Hallberg L, Bengtsson C, Lapidus L, et al. Screening for iron deficiency: an analysis based on bone-marrow examinations and serum ferritin determinations in a population sample of women. Br J Haematol. 1993; 85: 787-798.
- Andrews NC. Iron deficiency and related disorders. In: Greer JP, et al., eds. Wintrobe’s Clinical Hematology. 12th Philadelphia: Lippincott Williams & Wilkins; 2008. 810-834.
- 新津洋司郎 , 小船雅義 . 鉄欠乏性貧血 . 三輪血液病学 第 3 版 , 東京 ,文光堂 , 2006, 1000-1017.
- Kohgo Y, Niitsu Y, Kondo H, et al. Serum transferring receptor as a new index of erythropoiesis. Blood. 1987; 70: 1955-1958.
- Skikne BS, Flowers CH, Cook Serum transferrin receptor: a quantitative measure of tissue iron deficiency. Blood. 1990; 75: 1870-1876.
- Thomas DW, Hinchliffe RF, Briggs C, et al; British Committee for Standards in Guideline for the laboratory diagnosis of functional iron deficiency. Br J Haematol. 2013; 161: 639-648.
- Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood. 2015; 126: 1981-1989.
- Camaschella Iron-Deficiency Anemia. N Engl J Med. 2015; 373: 485-486.
コメント